99203 vs 99204: Understanding E/M Coding for Accurate Billing
In the complex world of medical billing, accurate coding is crucial for healthcare providers to receive proper reimbursement for their services. Among the many codes used, Evaluation and Management (E/M) codes are particularly important. Two commonly used E/M codes for new patients are 99203 and 99204. Understanding the differences between 99203 and 99204 is essential for proper coding and avoiding claim denials. This article will delve into a detailed comparison of these two codes, helping healthcare professionals differentiate between them and ensure accurate billing practices.
What are E/M Codes?
Evaluation and Management (E/M) codes are a set of Current Procedural Terminology (CPT) codes used to report the services provided by physicians and other qualified healthcare professionals during patient encounters. These codes encompass a wide range of services, including office visits, hospital visits, consultations, and emergency department visits. They are a fundamental part of medical billing and are used to determine the appropriate reimbursement for the cognitive work involved in evaluating and managing a patient’s condition.
Introduction to 99203 and 99204
CPT codes 99203 and 99204 specifically apply to new patients in an office or other outpatient setting. A new patient is defined as someone who has not received any professional services from the physician or another physician of the same specialty and subspecialty who belongs to the same group practice within the past three years. These codes are differentiated based on the level of medical decision-making and the amount of time spent with the patient. Choosing between 99203 and 99204 requires careful consideration of the components of the patient encounter.
Key Components of E/M Coding
Before diving into the specifics of 99203 and 99204, it’s important to understand the key components that determine the appropriate E/M code. These components include:
- History: This refers to the patient’s medical history, including chief complaint, history of present illness (HPI), past medical history, family history, and social history.
- Examination: This involves the physician’s physical examination of the patient, which can range from a problem-focused exam to a comprehensive exam.
- Medical Decision Making (MDM): This reflects the complexity of the physician’s thought process in evaluating the patient’s condition, considering differential diagnoses, and determining the appropriate management plan.
- Time: For some E/M codes, time can be a determining factor, especially when counseling and coordination of care dominate the encounter.
Detailed Comparison: 99203 vs 99204
Now, let’s compare 99203 and 99204 across the key components to understand their differences:
History
- 99203: Requires a detailed history. This typically includes an extended HPI, a problem pertinent system review (ROS), and a pertinent past, family, and/or social history (PFSH).
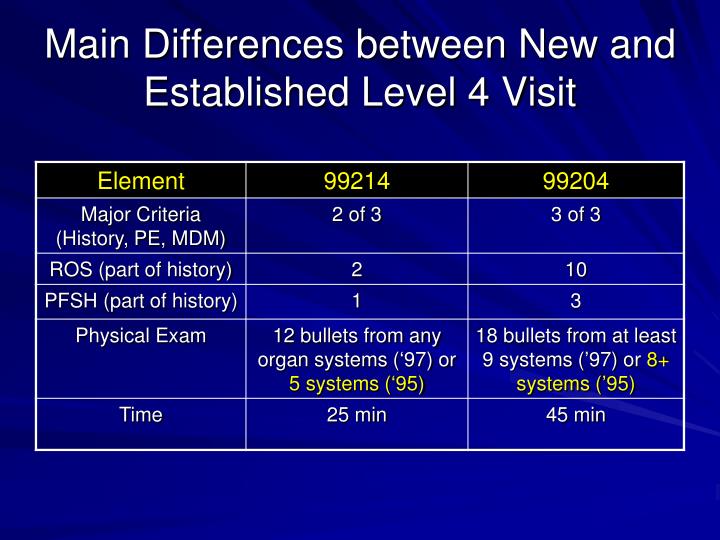
- 99204: Requires a comprehensive history. This means an extended HPI, a complete ROS, and a complete PFSH.
Examination
- 99203: Requires a detailed examination. This involves an extended examination of the affected body area(s) and other symptomatic or related organ system(s).
- 99204: Requires a comprehensive examination. This is a general multi-system examination or complete examination of a single organ system.
Medical Decision Making (MDM)
- 99203: Requires moderate complexity MDM. This involves multiple diagnoses or management options, a moderate amount of data to be reviewed, and a moderate risk of complications or morbidity.
- 99204: Requires moderate complexity MDM. This involves multiple diagnoses or management options, a moderate amount of data to be reviewed, and a moderate risk of complications or morbidity.
Time
- 99203: Typical time is 30-44 minutes.
- 99204: Typical time is 45-59 minutes.
When to Use 99203
Use 99203 when the new patient encounter involves a detailed history and examination, along with moderate complexity medical decision-making. This code is appropriate when the patient presents with a condition that requires a thorough evaluation but does not necessitate a comprehensive assessment of all aspects of their medical history and physical condition. For example, a patient presenting with a new onset of back pain requiring a detailed musculoskeletal examination and moderate complexity decision-making might warrant the use of 99203. The typical time associated with 99203 is 30-44 minutes.
When to Use 99204
Use 99204 when the new patient encounter involves a comprehensive history and examination, along with moderate complexity medical decision-making. This code is suitable for patients with more complex medical issues or those requiring a more thorough evaluation due to multiple comorbidities or a complicated medical history. For instance, a patient with a history of diabetes, hypertension, and hyperlipidemia presenting for a comprehensive evaluation of their overall health status and management of their chronic conditions would likely qualify for 99204. The typical time associated with 99204 is 45-59 minutes.
Examples to Illustrate the Difference
Let’s consider a couple of examples to further illustrate the differences between 99203 and 99204:
Example 1: A 35-year-old new patient presents with complaints of persistent headaches. The physician performs a detailed history, including the characteristics of the headaches, associated symptoms, and relevant past medical and family history. The physical examination includes a neurological assessment and examination of the head and neck. The physician considers several possible diagnoses, such as tension headaches, migraine headaches, and sinus headaches, and orders some tests to rule out other potential causes. The medical decision-making is of moderate complexity. The total time spent with the patient is 40 minutes. In this case, 99203 would be the appropriate code.
Example 2: A 60-year-old new patient with a history of heart disease and diabetes presents for a comprehensive evaluation. The physician obtains a comprehensive history, including a detailed review of all body systems, past medical history, family history, and social history. The physical examination is also comprehensive, covering multiple organ systems. The physician reviews the patient’s medications, discusses lifestyle modifications, and orders several lab tests and imaging studies. The medical decision-making is of moderate complexity, considering the patient’s multiple chronic conditions. The total time spent with the patient is 55 minutes. In this case, 99204 would be the appropriate code.
Common Mistakes to Avoid
Accurate coding requires attention to detail and a thorough understanding of the coding guidelines. Here are some common mistakes to avoid when choosing between 99203 and 99204:
- Upcoding: Selecting a higher-level code (e.g., 99204) when the documentation only supports a lower-level code (e.g., 99203). This can lead to overbilling and potential audits.
- Downcoding: Selecting a lower-level code when the documentation supports a higher-level code. This can result in underpayment for the services provided.
- Inadequate Documentation: Failing to document all the necessary components of the E/M service, such as the history, examination, and medical decision-making. Thorough documentation is essential to support the code selected.
- Ignoring Time: Not considering the total time spent with the patient, especially when counseling and coordination of care dominate the encounter.
Tips for Accurate Coding
To ensure accurate coding and avoid errors, consider the following tips:
- Review the Coding Guidelines: Familiarize yourself with the CPT coding guidelines for E/M services, including the definitions of key terms and the requirements for each code level.
- Document Thoroughly: Document all the necessary components of the E/M service, including the history, examination, and medical decision-making. Be specific and detailed in your documentation.
- Use a Coding Tool: Consider using a coding tool or software to assist with code selection. These tools can provide guidance and help ensure accuracy.
- Seek Education and Training: Participate in continuing education and training programs to stay up-to-date on the latest coding guidelines and best practices.
- Consult with a Coding Expert: If you have questions or concerns about coding, consult with a certified coding expert or auditor.
Impact of Coding Accuracy on Reimbursement
The accuracy of E/M coding directly impacts the reimbursement received by healthcare providers. Incorrect coding can lead to claim denials, reduced payments, and potential audits. By understanding the differences between codes like 99203 and 99204 and following proper coding guidelines, providers can ensure that they are appropriately compensated for their services. [See also: E/M Coding Updates for 2024]
Conclusion
Choosing between 99203 and 99204 requires a careful evaluation of the patient’s history, examination findings, and the complexity of medical decision-making. By understanding the nuances of these codes and following the coding guidelines, healthcare providers can ensure accurate billing and receive appropriate reimbursement for their services. Accurate coding is not only essential for financial success but also for maintaining compliance and providing quality care. Remember to focus on thorough documentation and continuous learning to stay proficient in E/M coding. Properly distinguishing between 99203 and 99204 is a cornerstone of efficient and ethical medical billing practices.
